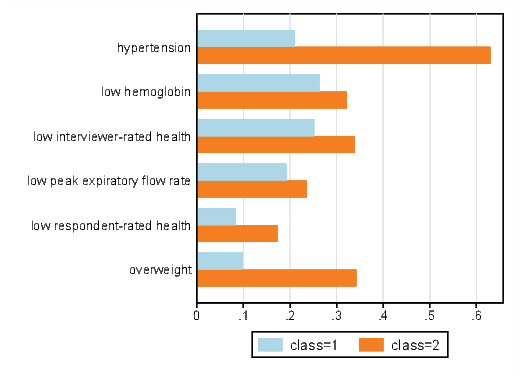
Figure 1: Rates of Low Health by Migrant and Flood Status

THE EFFECTS OF INTERNAL MIGRATION ON
HEALTH OF ADULTS IN INDONESIA
Partha Deb
Tamara Gurevich
ECONOMICS WORKING PAPER SERIES
Working Paper 2017–05–B
U.S. INTERNATIONAL TRADE COMMISSION
500 E Street SW
Washington, DC 20436
May 2017
This article is based on research for doctoral dissertation. Office of Economics working papers are the result of ongoing professional research of USITC Staff and are solely meant to represent the opinions and professional research of individual authors. These papers are not meant to represent in any way the views of the U.S. International Trade Commission or any of its individual Commissioners. Working papers are circulated to promote the active exchange of ideas between USITC Staff and recognized experts outside the USITC and to promote professional development of Office Staff by encouraging outside professional critique of staff research. Please address all correspondence to Tamara.Gurevich@usitc.gov.
The Effects of Internal Migration on Health of Adults in Indonesia
Partha Deb, Tamara Gurevich
Office of Economics Working Paper 2017–05–B
May, 2017
Abstract
In this paper we quantify effect of migration on health using a potential outcomes framework design that exploits exogenous impacts of floods on migration. We focus on six often-used measurements of physical and general health that are potentially modifiable over short periods of time. We construct a latent class model of the joint probabilities of the six health measures in which individuals are assumed to belong to one of a small number of (latent) health-types or classes. The class probabilities are modeled as being individual-specific. We estimate the model using data from the Indonesian Family Life Survey, an ongoing longitudinal survey of households and individuals in Indonesia. We find that migration last year has no effect on health, and that individuals who migrated two or more years ago as a result of a flood are 20 percent more likely to be in poor health than their non-migrant counterparts.
Partha Deb, Hunter College
partha.deb@hunter.cuny.edu
Tamara Gurevich, USITC
tamara.gurevich@usitc.gov
The United Nations estimates that in 2010 over 200 million people were living outside of their country of birth. Nearly four times as many people — almost 750 million — were internal migrants, relocating to other regions of their home country (UNDP, 2009). Lifetime internal migration estimates for developed countries show that some 255 million people live of outside their region of birth; nearly twice as many people — 505 million — migrated in the developing world (?). Furthermore, these numbers are expected to rise reflecting increases in future voluntary migration and involuntary displacement.
Migration has important implications for human development. On a macroeconomic level, integrating an increasing number of migrants may present social and economic challenges for governments and policy-makers in both developing and developed countries, however, the developing countries will face a greater difficulty since the number of migrants within developing countries is large and available resources are relatively scarce. Mohapatra et al. (2010) identify a number of social and economic challenges facing developing and developed countries as they try to integrate an ever increasing number of migrants. These include increased income inequality between migrant-sending and -receiving regions, higher burden on public services, stiffer job competition, and social tensions in migrant-receiving communities.
On the microeconomic side, individuals and households will likely encounter problems adopting to their new surroundings. Abbas and Varma (2014) discuss individual challenges, namely restricted access of recent migrants to housing, financial services and social programs. Further, the authors note that cultural and linguistic differences between sending and receiving regions may lead to harassment and political exclusion of migrants.
One important aspect of migrant well-being is migrants’ health. Good health is crucial for the ability to successfully adjust to new surroundings and become a productive member of society in a destination community. Therefore, if migrants have specialized health needs compared to natives at destination locations, understanding health consequences of migration is important to migrants, health professionals, and policy makers alike.
There is a long established, but relatively sparse literature on the effect of migration on health. This literature primarily addresses questions of post-migration adaptation and the role of remittances in health outcomes of migrants’ family members that remain in the origin communities. Only a handful of studies look at the effects of relocation on physical health of migrants. To a large extent this lack of scholarly research has to do with data limitations (Massey et al. (2010); Schenker et al. (2014)).
Studies that do focus on physical health usually look at a limited number of very specific measures of health and find that there are ambiguous effects of migration on health. Depending on measures (health outcomes) used, migration can have positive, negative or no effect on health at all. For example, in one paper, Lu (2010) finds that health of the same individuals may improve, deteriorate, or remain unchanged depending on how the author measures health.1
In addition, health selectivity of migrants — a hypothesis stating that individuals with higher initial stock of health are more likely to become migrants that is addressed in the healthy migrant literature — often masks potentially large negative effects of migration-correlated stressors, such as loss of familiar network, harsh working conditions, and environmental pressure on migrants’ physical health.2
Health status, however, is a complex conceptual construct. Its measurements are inherently multidimensional with broad classifications being along physical and mental health dimensions as well as biological measurement, physical impairment, and self-perceived status dimensions. Even within each of those dimensions, there are numerous measurements of health status, some substitutes, others complements for each other. Therefore, it is not surprising that the empirical evidence on the effects of migration on health is mixed.
Previous studies suggest several reasons why migration may lead to changes in migrants’ health. First, lack of familiarity with health systems in destination locations may result in limited access to health care services even in absence of legal restrictions, thus leading to health deterioration (Norredam, 2011). Second, health care professionals are often unaware of specific health needs of migrants, thus delaying proper diagnosis and treatment of migrant-specific ailments, which also adversely affects migrants’ health (Hansen and Donohoe, 2003). Lastly, stress associated with acculturation and adaptation to destination lifestyle often leads to uptake in unhealthy behaviors such as smoking and unhealthy diet (Renzaho and Burns (2006); Bosdriesz et al. (2013)). On the other hand, increased income and wealth may have positive effect on migrants’ health (LaLonde and Topel (1997); McKenzie et al. (2006)).3
In this paper, we quantify the effect of migration on physical health. We account for potential selectivity of health in migration using a potential outcomes framework of Athey and Imbens (2006) to disentangle health-selectivity of migrants from causal effects of migration. We use data on six measurements of physical and general health that are potentially modifiable over short periods of time (e.g., less than five years). These variables are all included in the “Global Reference List of Core Health Indicators” published by the World Health Organization (2015), a universal list of indicators “prioritized by the global community to provide concise information on the health situation and trends, including responses at national and global levels”.4 These six measures have well defined clinical cutoffs and are widely used in epidemiological and health economics studies.
We depart from the existing literature on the effects of migration on health in the way we model health outcomes. In order to preserve the richness of health information available in the data and to allow for potential correlation among different measures of health of the same individual, we assign individuals to two health classes — “good” and “poor” health — using Grade of Membership framework of Manton and Woodbury (1982) that allows for estimation of probability an individual is “healthy” given the individual’s health measures as well as other individual, household, and community characteristics. In doing so, we are able to quantify the effect of migration on a more comprehensive measure of health.
We construct a latent class model of the joint probabilities of the six health measures in which individuals are assumed to belong to one of a small number of (latent) health-types or classes. Thus, our model acknowledges the commonalities of the measurements while allowing for potential substitutability. Each latent class is associated with a probability and these class probabilities sum to one over the latent classes. The class probabilities are modeled as being individual-specific; i.e., they are functions of individual characteristics. This latent class model is closely related to the Grade of Membership (GoM) model of Manton and Woodbury (1982).
While the GoM method is similar to other data reduction models, such as Factor Analysis, Principle Components Analysis, and Multiple Indicator, Multiple Cause, this method is non-parametric; it does not rely on underlying distributional assumptions regarding individuals’ health when assigning individuals into health classes. Furthermore, GoM method takes into account individual heterogeneity when assigning respondents into discrete groups. This methodology allows for partial membership along different health dimensions, constructing a proximity measure between an respondent and a pure health type. Since only few people can be classified as perfectly healthy or completely unhealthy, GoM methodology offers additional advantages over other data reduction models (Portrait et al., 1999).
In order to reduce concerns about voluntary nature of migration, we incorporate recent local floods in potential outcomes framework of Athey and Imbens (2006) into our model. The vector of covariates in the class probability equation includes indicators for whether an individual migrated in the recent past, indicators for whether an individual was affected by a flood in the recent past, and interactions of migration and flood indicators. The coefficients on migration indicators account for possible self-selection into migration based on pre-migration health status. The indicators for floods account for possible health effects of exposure to floods. The interaction variables compare migrants who were pushed to migrate because of a recent flood to individuals who migrated from communities not affected by floods, and those who did not migrate at all. Thus, the coefficients on the interaction terms have a difference-in-difference interpretation (Athey and Imbens (2006); Puhani (2012)).
Confidence in the causal interpretation of the interaction of migration status and exposure to floods is based on two features of floods, combined with our focus on physical aspects of human health. First, conditional on geographic characteristics of each location, the timing of floods is essentially random. Second, while research indicates that there are some effects of floods on physical health of survivors, namely increase in diarrheal disease, mosquito-borne diseases, and upper respiratory infections, these effects are short lived (Ahern et al. (2005); Morgan et al. (2005)). Therefore, we can assume that floods don’t have a long lasting impact on individuals’ physical health. On the other hand, recent floods in origin communities do have an effect on subsequent migration probability (Kuhn, 2005).
We estimate our model using data from Indonesia. We select Indonesia because of its large population size, high rates of internal migration, geographic and social diversity, and high prevalence of flood events.5 We use the Indonesian Family Life Survey (IFLS), an ongoing longitudinal survey of households and individuals in Indonesia, representative of 83% of population of the country. Since its inception in 1993, this survey has been used in several hundred peer-reviewed papers.6 IFLS is unique in the way it treats migrants. It is designed to locate migrants following a move, thus greatly reducing migration-related sample attrition and allowing us to compare health of migrants and non-migrants. Most other surveys do not track down migrants, thus limiting researchers’ ability to investigate the effects of migration on health.
We find evidence that migration negatively affects health, and this effect becomes pronounced two or more years following a move. Migrating two or more years ago as a consequence of a flood increases the probability of being in poor health by 12 percentage points, an increase of nearly 20%, comparable to a loss of an average of five years of life.7 Migration a year ago has a small and statistically insignificant effect on the probability of being in poor health.
The remainder of the paper is structured as follows. Section 2 presents background on Indonesia, an overview of the data, and summary statistics. Methodology is described in section 3. Section 4 presents results and section 5 concludes.
Indonesia, a former Dutch colony, is the fourth most populous country in the world, located in Southeast Asia.8 The country is an archipelago consisting of over 17,500 islands, of which about 6,000 are inhibited by some 300 ethnic groups speaking more than 700 different languages.
Indonesia is subdivided into 34 provinces and special regions consisting of regencies (Kabupaten). Each Kabupaten is further subdivided into districts (Kecamatan), which are further divided into villages and urban communities (Desa). Indonesia is a lower middle income country. GDP per capita, adjusted to purchasing power parity, is $5,200, which places Indonesia 158 in the world countries’ rating. Almost 40% of the labor force is employed in agriculture, with agriculture share of GDP at 14%.
Health care in Indonesia is provided by a combination of public and private clinics as well as NGOs. Until 2014 Indonesia did not have universal health coverage; individuals were left to purchase health insurance independently with a limited public provision for the poorest. Average life expectancy at birth between 1993 and 2007 was 67 years, total annual per capita health expenditure during the same period was around $25 US. Cardio-vascular diseases, lower respiratory infections, and chronic obstructive pulmonary disease account for nearly half of all death with stroke — the leading cause of death — claiming 21%.9. Hypertension and obesity are fairly common: 30% of Indonesians have raised blood pressure, over 25% are overweight or obese.10
Additionally, major health risks come from waterborne and vectorborne diseases: bacterial diarrhea, hepatitis A, typhoid fever, dengue fever, and malaria. All of these diseases can, to some extent, be associated with recent floods (?). The most common natural hazards threatening inhabitants of Indonesian islands are floods, droughts, tsunamis, earthquakes, volcanic eruptions and forest fires.11 In addition, Indonesians are exposed to environmental issues of water and air pollution in urban areas, and smoke and haze from forest fires.
In this study, we use the Indonesian Family Life Survey (IFLS), a periodic panel survey administered by RAND. There are currently four waves available, spanning years 1993–2007. The sample spreads across 13 of 32 provinces in Indonesia, but represents about 83% of population at the survey onset. The 1993 wave has over 33,000 people living in 7,224 households in 312 sample communities. The sample grows to over 50,000 people in 13,536 households by 2007.12 Recontact rate in each wave of the the survey is over 90%.
The unique feature of this dataset is that it provides detailed retrospective migration histories for all respondents age 12 and older, as well as a very high precision of post-migration follow-ups. This greatly reduces attrition due to out-migration and allows us to investigate the effects of migration to communities that are not in the IFLS sample on post-migration health. Average migration rate of all respondents age 15 and older in the IFLS is 6.25%, which is nearly identical to the rate found by Gray et al. (2009) using different data sources from Indonesia.
We build a person-year panel, spanning all sixteen years of the survey. There are over 26,000 migration instances during the survey years, 1.2% of which are out of a community that has experienced a flood in the previous calendar year.13 We restrict our sample to adults of ages 15 to 65. Furthermore, once we take into account information on between sample year migrations and their relationship to flood events, we focus on the years of the last three waves of the survey for which we have exact measurements of health variables. This results in an unbalanced panel of over seventy thousand person-wave observations.
Health of respondents is measured only at survey years. Children of sample household and individuals that enter the sample between two waves do not have previous health measures. For this reason, and to avoid sample attrition, we use only one health measurement per respondent. The study design described below allows us to look at a “cross-section” of health outcomes and draw inferences regarding between-wave health changes using potential outcomes framework of Athey and Imbens (2006).
We construct six dichotomous measures of health based on body mass index, systolic and
diastolic blood pressure, hemoglobin count, peak expiratory flow rate measuring lung
capacity, health status as reported by the interviewer, and self-reported health status. We
select cutoffs to distinguish normal health from poor health based on commonly used
clinical values. Specifically, we classify individuals as overweight if their BMI is 25
or
above.14
Almost 20% of total sample are individuals who are overweight or obese, as defined by BMI of at
least 30 .
Hypertension is defined as per American Medical Association, with abnormal values of
systolic blood pressure of at least 130, diastolic blood pressure of at least 90. Nearly half of
the individuals in the sample have hypertension. Lung capacity depends on an individual’s
gender, age, and height; functional deficiency is defined as having a lung capacity that is
below 80% of group-specific normal function (Roberts and Mapel, 2012). 20% of sampled
individuals have low lung capacity. Normal hemoglobin levels are gender specific.
National Heart, Lung, and Blood Institute states that normal cutoffs are at least
for women
and at least
for men. Nearly 30% of sampled individuals have low hemoglobin. Two additional measures
are based on self-reported health status and on interviewers’ observations about the
respondents. 12% of respondents say the are unhealthy, while interviewers report nearly
30% of respondents being less healthy than the comparison group. Summary statistics
of these variables by survey year are shown in Table 2. In addition, Figure 1
shows rates of these poor health indicators by migrant status and exposure to
floods.
We define two indicators of migration status – whether a person migrated in the year before the survey, and whether a person migrated two or more years before the survey. We also define two indicators of exposure to floods – whether a person was exposed to a flood two years prior to the survey, and whether a flood exposure occurred three or more years prior to the survey. The indicator for migration a year prior is interacted with exposure to a flood two years ago. The indicators for migration two or more years prior is interacted with exposure to a flood three or more years ago.
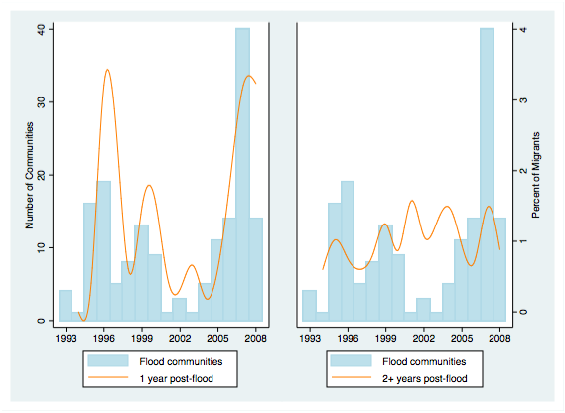
Figure 2 shows relationship between flood occurrences and flood-related migrations. Blue bars in both panels correspond to number of communities that experienced floods at any given year. In most years, 3–5% of sample communities experience a flood. The orange line in the left panel shows percent of all migrants that left a community that experienced a flood in the year prior to migration. For example, about 3% of all migrants in 1996 left a community that had a flood in 1995. The orange line in the right panel shows similar statistics, but for migrants leaving a community that experienced a flood two or more years prior to migration. There is a clear correlation between number of communities experiencing floods and percent of migrants leaving flood-affected communities a year later. This correlation is much weaker two or more years following a flood.15
Additional controls include socio-economic measures for individuals and households that are generally associated with migration: age, gender, level of education, marital status, and level of household wealth proxied by house ownership. We also include controls for original community location and other community characteristics: an indicator for urban and shore status of the community, its population size, distance to post office, and proportion of community population with access to telephones.
On average, migrants are younger and better educated than non-migrants. Migrants are more often male and not married, coming from households that are less likely to own a house. While there is virtually no difference between proportion of migrants and non-migrants in urban and shore locations, floods are somewhat more likely to hit urban areas and areas located on shores. Flood and non-flood communities are very similar along other dimensions. Tables 3 and 4 show these and other mean characteristics by migrant and flood status, and by survey year respectively.
Consider a design in which there is a binary migration indicator (with denoting the treatment group), a binary flood indicator (with denoting exposure to a flood) and denoting a set of control covariates. Then, using the potential outcomes framework, Athey and Imbens (2006) show that under assumptions of flood exogeneity and potential migrant self-selectivity the treatment effect in a potential outcomes model can be written as
where and denote the potential outcomes with and without treatment respectively.16 Envision as a latent measure of the likelihood of poor health, determined by a latent class model described below. In a nonlinear model parameterized with a linear index of covariates and parameters such that
Puhani (2012) shows that when ,
and
when , so that the sign of is the same as the sign of . Therefore, one can assess whether a treatment effect exists (and is statistically significant) by examining the coefficient on the interaction term in the regression specification, similar to treatment effect interpretation in difference-in-difference (DiD) models. In this framework, the treatment effect is given by
We begin with a set of observed outcomes that describe an underlying health concept. Each particular outcome is not sufficient to fully describe the underlying concept. However, taken together these variables can better summarize all available information about an individual’s unobserved health. The method adopted here is closely related to the Grade of Membership (GoM) model of Manton and Woodbury (1982) and is a nonparametric characterization of the latent construct. It allows for partial participation of an individual in each of the outcomes, recognizing that individuals can have different health conditions.
Following Portrait et al. (1999), consider a set of binary indicators, , that are the observed measurements of a common latent construct. Each of these measurements only partially characterizes the latent construct; in fact, all the the measurements, taken together, need not fully characterize the construct. if a respondent has a condition and otherwise. An individual that exhibits only symptoms of a single condition would be a “pure type”, using the language of the GoM model. We can measure the extent of proximity of each respondent to the pure types using weights that are constrained to fall between 0 and 1 and sum to 1 over all profiles; the respondents’ health conditions are then represented by a convex combination of the pure type profiles. Associated with each of these binary indicators is a probability that an individual exhibits symptoms of a health condition , and the joint probability associated with a higher value of the latent construct is given by .
A very general latent class model can be specified as follows. Suppose that there are classes (types) of individuals, with associated measurement probabilities given by for and is the probability that an individual belongs to class with .
Assume that the measurement probabilities are constant across individuals in a given class, i.e., and let
where denotes the multinomial logit function. Let be the baseline (omitted) category without loss of generality. Although this model is not completely general, it is considerably more parsimonious than the grade of membership model and gives us the ability to understand the determinants of the distribution of class probabilities within the context of the model.17
The contribution of an individual to the likelihood function is
and the overall log likelihood is
We estimate this model using maximum likelihood. Standard errors are adjusted for clustering at the household level.
To be more precise, we specify the class probability function as
where denotes that migration occurred last year, denotes migration occurred two or more years ago (but after the previous wave of data collection), denotes that the individual was exposed to a flood two years ago, denotes that the individual was exposed to a flood three or more years ago. In our empirical analysis, we find that the distribution of health status can be adequately described with two latent classes, so specializes to a logit function . The treatment effects, measured as changes in the probability of being in class 2 are given by
and
In most nonlinear models, as in our latent class model, it is not possible to “sweep out” unobserved group-level characteristics using the usual fixed effects time differencing technique, a within transformation, as one would in the linear model and some nonlinear models. Mundlak (1978) and Chamberlain (1984) note that, in the linear regression model, the fixed-effects (within) estimator produces the same coefficients as an OLS estimator in which the set of regressors includes group-level means of all the individual-level covariates in the regression specification. Taking this idea, they suggest that including group-level means as covariates in nonlinear models could ameliorate confounding caused by group-level characteristics. Therefore, in order to control for group-level fixed effects, in addition to estimating a latent class model that includes no group-level controls, we estimate versions of the model with two sets of group-level covariates: first with household-level means, and second with region-level (Kabupaten) means.
In order to compare our results to those in the previous literature, we estimate several alternative model specifications. First, we estimate a set of six potential outcomes logit specifications, one for each of the six binary health measures used in the latent class model. We then allow for correlation of various health measures for an individual, estimating a multivariate probit model with the same health measures. Last, but not least, we estimate a control function specification in order to control for migration selectivity.18
Table 11 presents coefficients from the two class grade of membership model under a naive assumption that individuals do not self-select into migration based on their health. Since we assume no selection, we do not include flood terms and flood-migration interaction terms that are present in our main specification in order to ameliorate the selectivity problem. Standard errors are clustered on household level. The first column presents results of a specification that includes a full set of individual, household and community characteristics only. Second and third columns show results of specifications that include household- and region (Kabupaten)-level Mundlak terms respectively.
All individual-, household- and community-level controls shown in Table 11 have expected signs and significance. Older individuals are more likely to be in poor health as are residents of large and urban communities. Wealthier and more educated householders are more likely to be healthier. However, migration on its own is not a significant predictor of subsequent health. The estimated posterior probability of being in class 2 is slightly above 0.4, regardless of specification. The joint probability of being in poor health given membership in class 2 is almost 45 times that of the joint probability of being in poor health given membership in class 1. In addition, Figure 3 shows that each of the individual measures of poor health are more likely to be observed among individuals a posteriori assigned to class 2. Therefore, we label class 2 as “poor health”.
Table 12 presents coefficients and summary statistics of our main latent class model estimation. The first specification includes a full set of individual characteristics. The second and third specifications include household- and region (Kabupaten)-level Mundlak terms. As before, standard errors are clustered on household level. The estimated posterior probability of being in class 2 is approximately 0.4, regardless of specification. The joint probability of being in poor health given membership in class 2 is about 45 times that of the joint probability of being in poor health given membership in class 1. The coefficients on the interaction terms in Table 12 show that migration last year has no effect on health, and that individuals who migrated two or more years ago are significantly more likely to be in poor health as a result of the migration.
The top panel of Figure 4 shows the predicted probabilities for three groups, those who did not migrate because of a flood, those who migrated a year ago because of a flood and those who migrated two or more years ago because of a flood. The bottom panel shows the associated marginal effects of migration because of a flood. Migrating two or more years ago as a consequence of a flood increases the probability of being in poor health by 12 percentage points. Migration a year ago has a small and statistically insignificant effect on the probability on being in poor health.
We find no evidence of the healthy migrant effect. The coefficients on migration are, across the board, statistically insignificant and small. This finding is consistent with Rubalcava et al. (2008), who find limited evidence for health selection among Mexican migrants to the United States. There is, however, a substantial effect of recent floods on health. Individuals exposed to recent floods are more likely to be in poor health.
Turning to other covariates in the model, men, individuals with higher education and those who own a house are less likely to be in poor health. In contrast older people are more likely to be in poor health. Individuals who live in large towns and cities (Desa), and urban areas are more likely to be in poor health. These findings are consistent with results from literature on adult health.
Table 13 presents results of several robustness checks. All four specifications include region (Kabupaten)-level Mundlak terms and standard errors are clustered on household level. Column 1 presents specification that includes age-squared term. The results are as predicted by theory. Age-squared term is significant and the sign is opposite of that of the age term. Individual who migrated two or more years ago following a flood are more likely to be unhealthy. Floods last year positively affect the probability of being in poor health. Floods two or more years ago are significant at 10%. Males and wealthier individuals are less likely to be unhealthy, while older people and residents of large communities have lower probability of being in good health.
Column 2 of Table 13 shows results of specification that includes only adults between ages 20 and 65. All coefficients are similar in sign and significance to those presented in column 1. Column 3 of Table 13 presents results of estimation for adults ages 20 to 60 to check whether the results are driven by presence of elderly individuals in the sample. Results are across the board similar to those discussed before. Estimation of specification for females only is presented in column 4 of Table 13. Women who migrated two or more years ago as a result of a flood, those who are older and are residents of larger communities are more likely to be unhealthy.
Specification shown in Table 14 includes interaction terms of age with migration-flood interactions to control for possible differential effect of flood-induced migration on individuals of different ages. Migration following a flood does not affect the probability of being in poor health, however individuals who migrated two or more years ago following a flood are more likely to be in poor health. Floods a year ago have a positive and significant effect on probability of being in poor health. Males and younger respondents are more likely to be healthier, as are more educated and wealthier individuals. The interaction term is only significant for flood-induced migration that happened a year ago. Interaction two or more years after a flood-induced migration is not significant.
Table 5 presents key coefficients from a set of descriptive potential outcomes logit regressions for each of the six measures of poor health status. All specifications include a full set of individual characteristics. In addition, the specification in 6 includes household-level Mudlak terms; the specification in 7 includes region (Kabupaten)-level Mundlak terms. In all cases, standard errors are clustered on household level. The results show that there are small, sometimes positive and sometimes negative, and statistically insignificant treatment effects of migration last year. The coefficients on migration 2 or more years ago interacted with flood exposure are always positive and relatively large, but not statistically significant in most cases. Migration 2 or more years ago (interacted with flood exposure) makes hypertension significantly more likely. The consistent positive signs on the treatment coefficients on migration 2 or more years ago are suggestive, however, that migration may lead to poor health.
Table 8 presents key coefficients from a set of multivariate probit regressions. As before, all specifications include a full set of individual characteristics. In addition, the specification in 9 includes household-level Mudlak terms; the specification in 10 includes region (Kabupaten)-level Mundlak terms and standard errors are clustered on household level. Results are similar to those from a set of logit regressions presented in Tables 5—7 and described above. Note that in addition to hypertension, now migration 2 or more years ago (interacted with flood exposure) significantly increases probability an individual has high BMI. The signs on the treatment coefficients on migration 2 or more years ago are still positive, again suggesting that migration may lead to poor health.
One possible channel that explains such deterioration of health is change in socio-economic surroundings of migrants. Khan and Kraemer (2014) state that migrants are more likely to smoke, which in turn can cause decreased lung capacity and other diseases generally associated with smoking. Change in diet is another channel that can adversely influence health. Renzaho and Burns (2006) show that migrants from sub-Saharan Africa to Australia increase consumption of takeaway food, e.g. Pizza Hut and McDonalds, and this increase in high-fat high-calorie consumption is generally associated with increase in body weight. Finally, impaired access to health care and lack of awareness of specialized health needs of migrants among health professionals lead to late diagnosis and inappropriate treatment of migrant-specific ailments (Hansen and Donohoe, 2003). More generally, literature on international migration show that health and health behavior of immigrants deteriorate with duration of stay abroad (Abdaido-Lanza et al. (2005); Lara et al. (2005)). Applied to domestic migrants, this would further explain cumulative negative effect of migration on health.
In order to shed some light on reasons why health of migrants deteriorates even though fewer people move following floods, we compare health of migrants and non-migrants by flood status, gender, age and other socio-economic characteristics. Figure 1 presents a break-down of rates of low health by migrant status and flood status. In addition, we run a series of t-tests to evaluate whether migrants and non-migrants, disaggregated by flood exposure status, have similar health outcomes.19 The results are presented in Tables 15—20.
Column 1 of Tables 15—20 presents results of the t-tests for equality of means of health indicators by migrant status. Looking at post-exposure health, migrants who moved following floods are no different from those who stayed in affected communities along all six health dimensions. However, those who were not exposed to floods differ in health outcomes by migrant status. Migrants are less likely to have high BMI, hypertension, low peak expiratory flow rate, and low hemoglobin.
We further disaggregate our sample to look at health outcomes of migrants and non-migrants by flood status and gender. The results of t-tests for the equality of means for male and female migrants and non-migrants potentially exposed to floods are presented in column 2 of Tables 15—20. Health outcomes of migrants that have been exposed to floods do not vary by gender. However, there is gender difference among migrants that have not been exposed to floods. Men are less likely to be unhealthy along all dimensions except hypertension.
Column 3 of Tables 15—20 shows results of t-tests for mean age difference of migrants that were exposed to floods and those that were not. While there is still no difference in health outcomes for the individuals that were exposed to floods, among the respondents that were not exposed, younger migrants are less likely to have high BMI and hypertension. One important observation is that among migrants that were not exposed to floods, younger individuals are less likely to report low self-rated health status. This could be interpreted as further evidence to support health selectivity in migration, underlining the importance of correcting for such selectivity.
Finally, we run one last series of t-tests, looking at migrant-sending summaries by household wealth, proxied here by ownership of a house. Individuals leaving wealthier households in presence of floods are no different in health outcomes from individuals leaving households that do not own their houses. However, in absence of floods, individuals leaving wealthier households are less likely to be overweight, but more likely to have low hemoglobin or appear to be less healthy to interviewers. One interpretation is that households that have higher wealth could afford to send out more migrants, even the ones that are on average less healthy. When households lose part of their wealth to floods, they can no longer send out migrants, thus rendering no difference in migrant-sending behavior among all households.
Overall, evidence presented above indicates that households and communities tend to send out fewer migrants following floods, in particular retaining younger, healthier men from wealthier households. The “labor-retention” hypothesis is one theory that would fit all these facts. Households and communities that typically send out migrants prefer to keep them at home to help with recovery efforts in the aftermath of floods, thus increasing labor demand for the exact individuals that would be most likely to move out in absence of floods.
This paper utilizes the GoM method to summarize health as a comprehensive measure that can be used to study the effects of migration on health. This method was designed by Manton and Woodbury (1982) for the purpose of categorizing complex multidimensional health concept, simultaneously identifying underlying dimensions of health and the degree to which individuals fit each of these dimensions. Using this method together with the IFLS data, we identify two broad health classes – good and poor health – and examine the effects of migration on probability of an individual belonging to poor health class.
We depart from the existing literature on migration and health by simultaneously addressing the issue of potential migrants’ selectivity on health and treating health as multidimensional, as opposed to looking into each health measure separately. We use data on six available measures of various aspects of health to characterize the underlying health concept. In doing so, we are able take into account the fact that an individual’s health cannot be described by a series of dichotomous outcomes.
We show that migration affects comprehensive health in an adverse way, and that the negative effects of migration on health accumulate over time. While migrants are as likely to be in poor health as non-migrants a year after a migration, two or more years later migrants are significantly more likely to be in worse health. Our findings align with several strands of literature on international migration and the subsequent health outcomes.
Migration is projected to increase in the coming decades in response, in part, to climate change (Drabo and Mbaye, 2011) and civil unrest, as is already evident in Europe and the Middle East. This will put increased pressure on health systems of destination locations, while subjecting an increasing number of people to migration-related health risks. Our results highlight the need for migrant-specific health policies that could help alleviate stress to health care systems of the receiving communities, and increase productivity and quality of life of migrant populations. Health care professionals need be made aware of migrant-specific maladies and appropriate testing and treatment procedures. Thus, the emphasis should be placed on further understanding of the causes of migrants’ health deterioration in order to reduce the health burden of migration.
| Disaster | Number of | Number of | Number of | Number of | Total Number | Total Damages |
| Type | Incidents | Deaths | Injured | Homeless | Affected | in 000 $U.S. |
| Flood | 62 | 2,985 | 1,795 | 25,235 | 4,690,805 | 2,268,276 |
| Earthquake | 45 | 174,367 | 152,613 | 1,397,288 | 5,331,126 | 8,830,676 |
| Landslide | 27 | 1,088 | 393 | 34,855 | 332,329 | 115,004 |
| Epidemic | 18 | 3,009 | 0 | 0 | 139,023 | 0 |
| Volcano | 16 | 102 | 139 | 0 | 134,031 | 0 |
| Wildfire | 8 | 243 | 470 | 0 | 3,034,470 | 9,315,800 |
| Drought | 2 | 672 | 0 | 0 | 1,080,000 | 89,000 |
| Storm | 2 | 4 | 0 | 0 | 3,715 | 0 |
Source: “EM-DAT: The OFDA/CRED International Disaster Database
| ||||||
www.em-dat.net - Universit Catholique de Louvain - Brussels - Belgium”
| ||||||
| 1997 | 2000 | 2007 | |
| Overweight | 16 | 17 | 24 |
| Hypertension | 59 | 44 | 41 |
| Low Peak Expiratory Flow Rate | 24 | 18 | 22 |
| Low Hemoglobin | 34 | 33 | 22 |
| Low Interviewer-Rated Health | 28 | 27 | 31 |
| Low Respondent-Rated Health | 11 | 12 | 13 |
% of total in each year
| |||
| Migrant | Never migrant | Flood | Never flood | |
| migrated last year | 0.210 | 0.000 | 0.025 | 0.043 |
| migrated 2+ years ago | 0.557 | 0.000 | 0.059 | 0.115 |
| flood last year | 0.026 | 0.043 | 0.215 | 0.000 |
| flood 2+ years ago | 0.052 | 0.078 | 0.396 | 0.000 |
| male | 0.493 | 0.456 | 0.438 | 0.468 |
| age in years | 32.489 | 36.424 | 37.348 | 35.308 |
| no schooling | 0.022 | 0.095 | 0.083 | 0.081 |
| high school or higher education | 0.558 | 0.368 | 0.375 | 0.410 |
| married | 0.488 | 0.514 | 0.554 | 0.499 |
| owns a house | 0.635 | 0.836 | 0.816 | 0.794 |
| year is 2000 | 0.343 | 0.339 | 0.362 | 0.335 |
| year is 2007 | 0.508 | 0.404 | 0.358 | 0.438 |
| log(population in Desa) | 8.687 | 8.620 | 8.687 | 8.621 |
| proportion of households in Desa with phone | 0.015 | 0.012 | 0.015 | 0.012 |
| log(distance to post office) | 1.789 | 1.794 | 1.743 | 1.804 |
| Desa is urban | 0.476 | 0.447 | 0.544 | 0.432 |
| Desa is on the shore | 0.140 | 0.152 | 0.213 | 0.136 |
| 10,770 | 46,529 | 10,566 | 46,733 | |
| 1997 | 2000 | 2007 | |
| migrated last year | 0.030 | 0.046 | 0.039 |
| migrated 2+ years ago | 0.042 | 0.119 | 0.128 |
| flood last year | 0.048 | 0.041 | 0.034 |
| flood 2+ years ago | 0.077 | 0.103 | 0.046 |
| male | 0.444 | 0.464 | 0.472 |
| age in years | 36.906 | 35.526 | 35.127 |
| no school | 0.128 | 0.088 | 0.049 |
| high school or higher education | 0.314 | 0.383 | 0.471 |
| married | 0.577 | 0.531 | 0.454 |
| own a house | 0.822 | 0.805 | 0.779 |
| log(population in Desa) | 8.555 | 8.682 | 8.637 |
| proportion of households in Desa with phone | 0.006 | 0.011 | 0.018 |
| log(distance to post office) | 1.156 | 2.587 | 1.512 |
| Desa is urban | 0.442 | 0.492 | 0.427 |
| Desa is on the shore | 0.131 | 0.142 | 0.167 |
| 13,581 | 19,468 | 24,250 | |
| overweight | hypertension | low | low | low intrvr | low respdnt | |
| PEFR | hemoglobin | rating | rating | |||
| migrated with flood last year | 0.098 | -0.140 | 0.170 | -0.004 | -0.019 | -0.062 |
| (0.318) | (0.262) | (0.315) | (0.288) | (0.311) | (0.404) | |
| migrated with flood 2+ years ago | 0.239 | 0.480*** | 0.249 | 0.226 | 0.105 | 0.022 |
| (0.172) | (0.140) | (0.196) | (0.138) | (0.159) | (0.202) | |
| overweight | hypertension | low | low | low intrvr | low respdnt | |
| PEFR | hemoglobin | rating | rating | |||
| migrated with flood last year | -0.106 | -0.132 | 0.202 | 0.055 | -0.108 | 0.066 |
| (0.317) | (0.272) | (0.299) | (0.303) | (0.314) | (0.443) | |
| migrated with flood 2+ years ago | 0.234 | 0.456*** | 0.196 | 0.191 | 0.002 | 0.073 |
| (0.154) | (0.138) | (0.187) | (0.152) | (0.175) | (0.215) | |
| overweight | hypertension | low | low | low intrvr | low respdnt | |
| PEFR | hemoglobin | rating | rating | |||
| migrated with flood last year | 0.179 | -0.169 | 0.036 | -0.083 | -0.215 | 0.025 |
| (0.323) | (0.263) | (0.330) | (0.296) | (0.315) | (0.411) | |
| migrated with flood 2+ years ago | 0.247 | 0.435*** | 0.231 | 0.237* | 0.136 | 0.136 |
| (0.169) | (0.140) | (0.203) | (0.139) | (0.169) | (0.199) | |
| overweight | hypertension | low | low | low intrvr | low respdnt | |
| PEFR | hemoglobin | rating | rating | |||
| migrated with flood last year | 0.024 | -0.148 | 0.131 | 0.031 | 0.034 | -0.082 |
| (0.175) | (0.162) | (0.178) | (0.162) | (0.172) | (0.215) | |
| migrated with flood 2+ years ago | 0.168* | 0.201** | 0.075 | 0.054 | -0.019 | 0.003 |
| (0.088) | (0.081) | (0.082) | (0.081) | (0.172) | (0.102) | |
| overweight | hypertension | low | low | low intrvr | low respdnt | |
| PEFR | hemoglobin | rating | rating | |||
| migrated with flood last year | -0.080 | -0.067 | 0.146 | 0.053 | -0.026 | -0.019 |
| (0.178) | (0.168) | (0.169) | (0.172) | (0.175) | (0.230) | |
| migrated with flood 2+ years ago | 0.118 | 0.096 | 0.022 | 0.035 | -0.011 | -0.040 |
| (0.085) | (0.079) | (0.084) | (0.092) | (0.091) | (0.105) | |
| overweight | hypertension | low | low | low intrvr | low respdnt | |
| PEFR | hemoglobin | rating | rating | |||
| migrated with flood last year | 0.061 | -0.155 | 0.070 | -0.083 | -0.061 | -0.012 |
| (0.178) | (0.165) | (0.183) | (0.296) | (0.184) | (0.216) | |
| migrated with flood 2+ years ago | 0.016* | 0.170** | 0.043 | 0.060 | 0.091 | -0.036 |
| (0.090) | (0.081) | (0.084) | (0.081) | (0.095) | (0.103) | |
* .1; **
.05; ***
.01
* .1; **
.05; ***
.01
* .1; **
.05; ***
.01
* .1; **
.05; ***
.01
* .1; **
.05; ***
.01
| Migrant | Male | Age | Own house | |
| Flood | 0.069 | 0.082 | 0.002 | 0.052 |
| (0.043) | (0.082) | (0.004) | (0.095) | |
| No Flood | 0.020** | 0.072*** | 0.007*** | 0.044*** |
| (0.008) | (0.016) | (0.001) | (0.017) | |
* p 0.1; ** p 0.05; *** p 0.01
| ||||
Differences in means between non-migrants (0) and migrants (1)
| ||||
Differences in means between female (0) and male (1), migrants only
| ||||
Differences in mean age, migrants only
| ||||
Differences in house ownership status, migrants only
| ||||
| Migrant | Male | Age | Own house | |
| Flood | 0.026 | -0.159 | 0.009 | -0.029 |
| (0.056) | (0.111) | (0.005) | (0.119) | |
| No Flood | 0.102*** | -0.136*** | 0.012*** | 0.010 |
| (0.010) | (0.019) | (0.001) | (0.019) | |
* p 0.1; ** p 0.05; *** p 0.01
| ||||
Differences in means between non-migrants (0) and migrants (1)
| ||||
Differences in means between female (0) and male (1), migrants only
| ||||
Differences in mean age, migrants only
| ||||
Differences in house ownership status, migrants only
| ||||
| Migrant | Male | Age | Own house | |
| Flood | 0.023 | 0.009 | -0.006 | -0.001 |
| (0.049) | (0.098) | (0.004) | (0.105) | |
| No Flood | 0.032*** | 0.050*** | 0.001 | -0.005 |
| (0.008) | (0.016) | (0.001) | (0.016) | |
* p 0.1; ** p 0.05; *** p 0.01
| ||||
Differences in means between non-migrants (0) and migrants (1)
| ||||
Differences in means between female (0) and male (1), migrants only
| ||||
Differences in mean age, migrants only
| ||||
Differences in house ownership status, migrants only
| ||||
| Migrant | Male | Age | Own house | |
| Flood | 0.012 | 0.179* | 0.004 | 0.061 |
| (0.052) | (0.098) | (0.005) | (0.113) | |
| No Flood | 0.054*** | 0.152*** | 0.001 | -0.037** |
| (0.009) | (0.018) | (0.001) | (0.018) | |
* p 0.1; ** p 0.05; *** p 0.01
| ||||
Differences in means between non-migrants (0) and migrants (1)
| ||||
Differences in means between female (0) and male (1), migrants only
| ||||
Differences in mean age, migrants only
| ||||
Differences in house ownership status, migrants only
| ||||
| Migrant | Male | Age | Own house | |
| Flood | 0.013 | 0.105 | 0.005 | -0.096 |
| (0.051) | (0.099) | (0.005) | (0.103) | |
| No Flood | 0.048*** | 0.045** | 0.001 | -0.063*** |
| (0.009) | (0.018) | (0.001) | (0.018) | |
* p 0.1; ** p 0.05; *** p 0.01
| ||||
Differences in means between non-migrants (0) and migrants (1)
| ||||
Differences in means between female (0) and male (1), migrants only
| ||||
Differences in mean age, migrants only
| ||||
Differences in house ownership status, migrants only
| ||||
| Migrant | Male | Age | Own house | |
| Flood | -0.051 | -0.006 | -0.005 | 0.055 |
| (0.046) | (0.093) | (0.004) | (0.102) | |
| No Flood | -0.002 | 0.012 | 0.003*** | 0.014 |
| (0.007) | (0.014) | (0.001) | (0.014) | |
* p 0.1; ** p 0.05; *** p 0.01
| ||||
Differences in means between non-migrants (0) and migrants (1)
| ||||
Differences in means between female (0) and male (1), migrants only
| ||||
Differences in mean age, migrants only
| ||||
Differences in house ownership status, migrants only
| ||||
Rameez Abbas and Divya Varma. Internal Labor Migration in India Raises Integration Challenges for Migrants, March 2014. URL http://www.migrationpolicy.org/article/internal-labor-migration-india-raises-integration-challenges-migrants. [Online; posted 3-March-2014].
A. F. Abdaido-Lanza, M. T. Chao, and K. R. Florez. Do Healthy Behaviors Decline with Greater Acculturation? Implications for the Latino Mortality Paradox. Social Science & Medicine, 61:1243–1255, 2005.
A F Abraido-Lanza, B P Dohrenwend, D S Ng-Mak, and J B Turner. The Latino Mortality Paradox: A Test of the “Salmon Bias” and Healthy Migrant Hypotheses. American Journal of Public Health, 89(10):1543–1548, 1999.
Mike Ahern, R. Sari Kovats, Paul Wilkinson, Roger Few, and Franziska Matthies. Global Health Impacts of Floods: Epidemiological Evidence. Epidemiological Reviews, 27:36–46, 2005.
Environmental Influences on Migration in Rural Ecuador, 2010. Annual Meeting of Population Association of America.
Mohamed Arouri, Cuong Nguyen, and Adel ben Youssef. Natural Disasters, Household Welfare, and Resilience: Evidence from Rural Vietnam. World Development, 70:59–77, 2015.
Susan Athey and Guido W. Imbens. Identification and Inference in Nonlinear Difference-in-Difference Models. Econometrica, 74(2):431–497, 2006.
Jizzo R. Bosdriesz, Nienke Lichthart, Margot I. Witvliet, Wim B. Busschers, Karien Stronks, and Anton E. Kunst. Smoking Prevalence among Migrants in the US Compared to the US-Born and the Population in Countries of Origin. PLOS One, 8(3), 2013.
Gary Chamberlain. Chapter 22: Panel Data. In Zvi Griliches and Michael Intriligator, editors, Handbook of Econometrics, pages 1247–1318. Elsevier Science, 1984.
Partha Deb and Pravin K. Trivedi. Demand for Medical Care by the Elderly: A finite Mixture Approach. Journal of Applied Econometrics, 12(3):313–336, 1997.
A. P. Dempster, N. M. Laird, and D. B. Rubin. Maximum Likelihood from Incomplete Data via the EM Algorithm. Journal of the Royal Statistical Society. Series B (Methodological), 39(1):1–38, 1977.
Alassane Drabo and Linguere Mously Mbaye. Climate Change, Natural Disasters, and Migration: An Empirical Analysis in Developing Countries. 2011.
Melissa M. Garrido, Partha Deb, Jr. James F. Burgess, and JOan D. Penrod. Choosing Models for Health Care Cost Analyses: Issues of Nonlinearity and Endogeneity. Health Services Research, 47(6):2377–2397, 2012.
Noreen Goldman, Anne R. Pebley, Mathew J. Creighton, Graciela M. Teruel, Luis N. Rubalcava, and Chang Chung. The Consequences of Migration to the United States for Short-Term Changes in the Health of Mexican Immigrants. Demography, 51:1159–1173, 2014.
Clark Gray, Elizabeth Frankenberg, Thomas Gillespie, Duncan Thomas, and Cecep S. Sumantri. Tsunami-induced Displacement in Sumatra, Indonesia. Marrakech, 2009. International Union for the Scientific Study of Population. URL http://iussp2009.princeton.edu/papers/90318.
Timothy Halliday. Migration, Risk, and Liquidity Constraints in El Salvador. Economic Development and Cultural Change, 25(5):893–925, 2006.
Eric Hansen and Martin Donohoe. Health Issues of Migrant and Seasonal Farmworkers. Journal of Health Care for the Poor and Underserved, 14(2):153–164, 2003.
John R. Harris and Michael P. Todaro. Unempoyment and Development: A Two-Sector Analysis. The American Economic Review, 60(1):126–142, 1970.
Nicole Hildebrandt, David J. McKenzie, Gerardo Esquivel, and Ernesto Schargrodsky. The Effects of Migration on Child Health in Mexico. Economia, 6 (1):257–289, 2005.
Graeme Hugo. Environmental Concerns and International Migration. International Migration Review, 30(1):105–131, 1996.
Stanislav V. Kasl and Lisa Berkman. Health Consequences of the Experience of Migration. Annual Reviews of Public Health, 4:69–90, 1983.
Md. Mubarak Hossain Khan and Alexander Kraemer. Are Rural-Urban Migrants Living in Urban Slums More Vulnerable in Terms of Housing, Health Knowledge, Smoking, Mental Health and General Health? International Journal of Social Welfare, 23:373–383, 2014.
Randal S. Kuhn. The Determinants of Family and Individual Migration: A Case-Study of Rural Bangladesh. Working Paper, 2005.
Robert J. LaLonde and Robert H. Topel. Economic Impact of International Migration and the Economic Performance of Migrants. In Mark R. Rosenzweig and Oded Stark, editors, Handbook of Population and Family Economics, pages 799–850. Elsevier Science, 1997.
M. Lara, C. Gamboa, M. I. Kahramanian, L. Morales, and D. Bautista. Acculturation and Latino Health in the United States: A Review of the Literature and its Sociopolitical Context. Annual Review of Public Health, 26:367–397, 2005.
Jane H. Lassetter and Lynn C. Callister. The Impact of Migration on the Health of Voluntary Migrants in Western Societies. Journal of Transcultural Nursing, 20 (1):93–104, 2009.
Yao Lu. Test of the ‘Healthy Migrant Hypothesis’: A Longitudinal Analysis of Health Selectivity of Internal Migration in Indonesia. Social Sscience and Medicine, 67:1331–1339, 2008.
Yao Lu. Rural-Urban Migration and Health: Evidence from Longitudinal Data in Indonesia. Social Sscience and Medicine, 70:412–419, 2010.
Kenneth G. Manton and Max A. Woodbury. A New Procedure for Analysis of Medical Classification. Methods of Information in Medicine, 21(4):210–220, 1982.
Kenneth G. Manton, Eric Stallard, and Max A. Woodbury. Applications of the Grade of Membership Technique to Event History Analysis: Etensions to Multivariate Unobserved Heterogeneity. Mathematical Modelling, 7:1375–1391, 1986.
Kenneth G. Manton, Max A. Woodbury, James C. Vertrees, and Eric Stallard. Use of Medicare Services Before and After Introduction of the Prospective Payment System. Health Services Research, 28(3):269–292, 1993.
Douglas S Massey. Immigration Statistics for the 21st Century. Annals of the American Academy of Political and Social Science, 631(1):124–140, 2010.
Douglas S. Massey and Kristin E. Espinosa. What’s Driving Mexico–U.S. Migration? A Theoretical, Empirical, and Policy Analysis. American Journal of Sociology, 102(4):939–999, 1997.
Douglas S. Massey, William G. Axinn, and Dirgha J. Ghimire. Environmental Change and Out-Migration: Evidence from Nepal. Population and Environment, 32(2):109–136, 2010.
Laura McKay, Sally Macintyre, and Anne Ellaway. Migration and Health: A Review of the International Literature. 2003.
David McKenzie, John Gibson, and Steven Stillman. How Important is Selection? Experimental vs. Non-Experimental Measures of the Income Gains from Migration. 2006.
Geoffrey McLachlan and David Peel. Finite mixture models. John Wiley & Sons, 2004.
J. Mincer. Family Migration Decisions. Journal of Political Economy, 86(5): 749–773, 1978.
Sanket Mohapatra, Dilip Ratha, and Elina Scheja. Impact of Migration on Economic and Social Development: A Review of Evidence and Emerging Issues. Technical report, Migration and Remittances Unit, World Bank, 2010.
Mark R. Montgomery and Paul C. Hewett. Urban Poverty and Health in Developing Countries: Household and Neighborhood Effects. Demography, 42(3): 397–425, 2005.
O. Morgan, M. Ahern, and S. Cairncross. Revisiting the Tsunami: Health Consequences of Flooding. PLoS Med, 2(6), 2005.
Yair Mundlak. On the Pooling of Time Series and Cross Section Data. Econometrica, 46(1):69–85, 1978.
Marie Norredam. Migrant’s Access to Healthcare. Danish Medical Bulletin, 58 (10):B4339, 2011.
France Portrait, Maarten Lindeboom, and Dorly Deeg. Health and Mortality of the Elderly: The Grade of Membership Method, Classification and Determination. Health Economics, 8:441–457, 1999.
Patrick A. Puhani. The Treatment Effect, the Cross Difference, and the Interaction Term in Nonlinear “Difference-in-Differences” Models. Economic Letters, 115:85–87, 2012.
Andre M.N. Renzaho and Cate Burns. Post-Migration Food Habits of Sub-Saharan African Migrants in Victoria: A Cross-Sectional Study. Nutrition & Dietetics, 63:91–102, 2006.
Melissa H. Roberts and Douglas W. Mapel. Limited Lung Function: Impact of Reduced Peak Expiratory Flow on Health Status, Health-Care Utilization, and Expected Survival in Older Adults. American Journal of Epidemiology, 176(2): 127–134, 2012.
Mark R. Rosenzweig and Oded Stark. Consumption Smoothing, Migration, and Marriage: Evidence from Rural India. The Journal of Political Economy, 97(4): 905–926, 1989.
Luis N. Rubalcava, Graciela M. Teruel, Duncan Thomas, and Noreen Goldman. The Healthy Migrant Effect: New Findings From the Mexican Family Life Survey. American Journal of Public Health, 98(1):78–84, 2008.
Sergio O. Saldaña-Zorrilla and Krister Sandberg. Spacial Econometric Model of Natural Disaster Impact on Human Migration in Vulnerable Regions of Mexico. Disasters, 33(4):591–607, 2009.
Marc B Schenker, Xòchitl Castañeda, and Alfonso Rodriguez-Lainz. Migration and Health: A Research Methods Handbook. University of California Press, Oakland, California, 2014.
Oded Stark and David E. Bloom. The New Economics of Labor Migration. American Economic Review, 75(2):173–178, 1985.
United Nations Development Program UNDP. Human Development Report 2009 — Overcoming Barriers: Human Mobility and Development. Technical report, 2009. URL http://hdr.undp.org/sites/default/files/reports/269/hdr_2009_en_complete.pdf.
Leah K. VanWey. Land Ownership as a Determinant of International and Internal Migration in Mexico and Internal Migration in Thailand. International Migration Review, 39(1):141–172, 2005.
J. Vearey and B. Wheeler. Migration and Health in SADC: A Review of the Literature, 2010.
Peter von Rooij. Labour and Social Trends in Indonesia 2011: Promoting Job-Rich Growth in Provinces. Technical report, International Labour Organization, 2012.
World Health Organization (WHO). Global Reference List of Core Health Indicators: Working Version 5. Technical report, Geneva, Switzerland, 2015. URL http://apps.who.int/iris/bitstream/10665/173589/1/WHO_HIS_HSI_2015.3_eng.pdf?ua=1.
Ben Wisner, Piers Blaikie, Terry Cannon, and Ian Davis. At Risk: Natural Hazards, People’s Vulnerability and Disasters. Routledge, 2004.
Dean Yang. Risk, Migration and Rural Financial Markets: Evidence from Earthquakes in El Salvador. Social Research, 73(3):955–992, 2008.
Yaohui Zhao. Labor Migration and Earnings Differences: The Case of Rural China. Economic Development and Cultural Change, 47(4):767–782, 1999.
1Lu (2010) is just one example of many with similar approach and findings. See Kasl and Berkman (1983), McKay et al. (2003), Lassetter and Callister (2009), and Vearey and Wheeler (2010) for a comprehensive literature review.
2Pre-migration health selectivity is well documented in literature on “healthy migrant hypothesis”. For more recent examples, see Rubalcava et al. (2008) and Lu (2010).
3Also see Goldman et al. (2014) for extended discussion.
4http://apps.who.int/iris/bitstream/10665/173589/1/WHO_HIS_HSI_2015.3_eng.pdf?ua=1
5An estimated 10% of population of Indonesia (about 23 million people) are internal migrants (? and Lu (2008)); floods are the most common natural disasters in Indonesia, accounting for 70% of all natural disasters (?).
6http://www.rand.org/labor/FLS/IFLS.html
7http://www.who.int/gho/countries/idn.pdf
8Here and further the background information on Indonesia is provided by the CIA World Fact Book last accessed on May 1, 2016 at https://www.cia.gov/library/publications/the-world-factbook/geos/print/country/countrypdf_id.pdf
9https://www.cdc.gov/globalhealth/countries/indonesia/
http://www.who.int/gho/countries/idn.pdf
10http://www.who.int/nmh/countries/idn_en.pdf
http://www.genre.com/knowledge/publications/uwfocus14-2-cheong-en.html
11EM-DAT: The OFDA/CRED International Disaster Database reports 62 major flood events in Indonesia during the period of 1993–2007. 4,690,805 individuals are estimated to have been affected by floods, with 2,985 dying as a result of a flood (0.064% of those affected). www.em-dat.net — Universit Catholique de Louvain — Brussels — Belgium.
12Sample grows because survey respondents marry partners that were initially out of sample. In addition, those sample household members who were under the age of 12 during initial sampling enter the following waves if old enough.
13Table 1 presents detailed summary of natural disasters affecting Indonesia between 1993 and 2007. Floods are the most common natural disasters, affecting most people and causing most damages excluding the 2004 Indian Ocean tsunami.
14Only a small proportion of the sample is underweight; those individuals are included in the normal weight group.
15Correlation values are 0.67 for the left panel, 0.15 for the right panel.
16Consider a population in which individuals can be described as migrant and non-migrant types that could be affected by a flood. Then, look at health of migrants, compared to non-migrants, in absence of treatment, the floods. Assuming that the same would hold for those in treatment group had they not been affected by a flood, estimate the counterfactual outcome distribution for treated and compare the estimated counterfactual distribution to the actual distribution to tease out the effect of migration on subsequent health using floods to reduce concerns about migrant selectivity.
17The estimated mixing probabilities in the grade of membership model can be used as the dependent variable in an auxiliary regression analysis to understand its determinants but this approach has all of the inherent issues in multi-step modeling procedures.
18Control function method is less reliable than the DiD specification described above. Due to non-linearity of the second stage regression and issues of timing of migration relative to flood measures and health measures, this specification produces noisy estimates. The results of the control function specification are not significant, but are similar in direction and magnitude to those of the DiD specification. For this reason, the DiD method is preferred, since results of the two estimations are comparable. Results the control function specification are omitted to conserve space.
19We allow for variances to differ by group.